Ririka MIURA*1, Rikei KOZAKAI*1, Susumu SUZUKI, PhD*1, 2, †Shinichiro TAKAHASHI, MD, PhD*1, 2
Cite
MIURA R, KOZAKAI R, SUZUKI S, TAKAHASHI S. Analysis of Incident/Accident Reportsin the Department of Clinical Laboratory at Tohoku Medicaland Pharmaceutical University Hospital:Effect of ISO 15189 Implementation on Medical Safety. Lab Med Int 2024; 3(1): 8-14. doi: 10.51041/lmi.3.1_8
Original
Lab Med Int 2024; 3(1): 8-14
†Correspondence: Division of Laboratory Medicine, Faculty of Medicine, Tohoku Medical and Pharmaceutical University, 1-15-1 Fukumuro, Miyagino-ku, Sendai 983-8536, Japan.
E-mail: shintakahashi”@”tohoku-mpu.ac.jp
Received July 5, 2023; accepted January 16, 2024
*1 Department of Clinical Laboratory, Tohoku Medical and Pharmaceutical University Hospital, 1-12-1 Fukumuro, Miyagino-ku, Sendai 983-8512, Japan
*2 Division of Laboratory Medicine, Faculty of Medicine, Tohoku Medical and Pharmaceutical University, 1-15-1 Fukumuro, Miyagino-ku, Sendai 983-8536, Japan
ABSTRACT
Objective: Managing the safety and security of medical treatment information is critical for every clinical department in a hospital, and improving safety and security management is increasingly emphasized. Our laboratory, the Department of Clinical Laboratory, Tohoku Medical and Pharmaceutical Hospital, acquired ISO 15189 accreditation in January 2019. We sought to assess the effect of ISO 15189 quality management on medical safety by analyzing incidents and accidents before 2017 and from ISO 15189 acquisition until 2022.
Methods: We assessed the classification of incident severity, the medical services in which incidents occurred, the specific laboratory test steps in which incidents occurred, the variety and number of recurrences, and the medical services in which recurrent incidents were observed.
Results: No accidents above level 3b were observed over the study period, and the total number of incidents decreased significantly after 2020. Level 1 incidents in particular decreased notably after 2021. Incidents that occurred during the night shift/day duty dramatically decreased after 2019 (2017–2018, 21 cases; 2019–2022, 10 cases, p < 0.001). The proportions of incidents by laboratory test step remained unchanged. The number of recurrent incidents was highest in 2018 (12 cases) and then gradually decreased (2019, eight cases; 2020, five cases; and 2021, one case). No recurrent cases were observed after 2022.
Conclusions: Implementing a quality management system that meets ISO 15189 standards is associated with fewer incidents, especially in night shift/day duty services. Reducing recurrent incidents may require additional time, even with the application of ISO 15189 systems.
〔Lab Med Int 2024; 3(1): 8-14〕
Key Words
incidents, ISO 15189, risk management, medical safety
I. Introduction
Achieving medical safety in all the medical departments of a hospital is very important. The 2007 medical service law enforced the preparation of guidelines not only for infection control, operational procedures for pharmaceutical medicines, and maintenance plans for medical equipment but also for medical safety 1). Therefore, guidelines to ensure medical safety are always required. The errors that occur in clinical diagnostic laboratories are suggested to be fewer than those that occur elsewhere in a hospital setting; however, even a low rate may reflect a large number of errors 2). Strengthening medical safety has been attracting attention as an approach to delivering conclusive and accurate clinical laboratory data to physicians 3, 4).
In Tohoku Medical and Pharmaceutical University Hospital, an incident report management system, e-power/CLIP (NSD Corp., Tokyo, Japan), has been used since January 2017. By allowing the rapid issue of incident reports, this system contributes to improving the quality of medical services. The following is an example of our practical use of the CLIP system. On 5 July 2021, a clinical specimen sent with a dumbwaiter from the central supply division was ignored for a period beyond that allowed from the time of specimen collection. As a result, the specimen had to be collected again. The CLIP system reported the event on the same day. On July 7, the Medical Safety Managing Department directed that posters displaying “No specimens” be posted on all of the dumbwaiter doors on each floor. On 15 July, a manager from each of the hospital’s wards and medical divisions participated in the monthly risk manager meeting and the incident was shared. In summary, only 2 days after the CLIP report, a quick fix was implemented through the collaboration of the Medical Safety Management and the Clinical Laboratory departments, and the poster was posted in all the divisions in the hospital within 8 days. Thereafter, no recurrence of the incident was reported. The CLIP system has enabled a rapid response and efficient communication to address incidents related to medical safety.
ISO 15189 is an international standard that specifies the requirements for quality management systems (QMS) that are specific to medical laboratories. The standard has been reported to play an important role in quality improvement and the prevention of examination errors 5, 6). Our laboratory, the Department of Clinical Laboratory at Tohoku Medical and Pharmaceutical Hospital, received ISO 15189 accreditation in January 2019 7). In this study, we examined the effects of ISO 15189 accreditation and CLIP management on the number and types of incidents. Specifically, we assessed the incident severity classification, the medical services and laboratory testing steps in which incidents occurred, the type and number of recurrences, and the medical services in which recurrences occurred in the fiscal years 2017 to 2022. Furthermore, we discuss the role and significance of ISO 15189 on QMS in the prevention of incidents.
II. Methods
Participants
We determined the number of tests conducted in the Department of Clinical Laboratory, Tohoku Medical and Pharmaceutical University Hospital. In total, 95 incident reports were delivered to the Medical Safety Management Department by the CLIP system between April 2017 and March 2023. The incident severity classification system recommended by the National University Hospital Council of Japan 8) was used, and the risk manager of the Medical Safety Management Department in our hospital objectively determined the final incident level using this classification system. For all of the incidents that occurred during the study period, we determined the incident severity classification, the medical services in which incidents occurred, the laboratory testing steps in which incidents happened, the type and number of recurrences, and the medical services in which recurrences occurred. The following were the numbers of incidents/total numbers of tests observed throughout the study period: 2017: 26/2,201,331, 2018: 27/2,301,813, 2019: 17/2,545,856, 2020: 10/2,670,728, 2021: 9/2,906,752, and 2022: 6/2,873,229.
Statistics
For statistical analysis of the transition of incident occurrence, we first prepared a cross-tabulation table for each fiscal year or setting. We then performed a chi-square test and residual analysis, and statistical significance was calculated. We compared the values for the 2017 or 2018 fiscal year with those for every year after 2019, using the above strategy (Figure 1). We noted the p-value when significance was shown (p < 0.05, p < 0.01, and p < 0.001). We used the Holm–Bonferroni method to calculate the revised p-value. In addition, the p-values (Figures 2 to 4) were calculated from adjusted residuals.
Ethics
We carefully considered personal information. This study focused on the details of the incidents and ignored the personal information of the persons who reported, caused, or suffered from the incidents. The study was approved by the Ethics Committee of the Tohoku Medical and Pharmaceutical University Hospital (2023-2-012). Informed consent for the handling of personal information and the opportunity to deny participation was obtained in the form of an opt-out sent by e-mail to the Department of Clinical Laboratory staff.
III. Results
Annual change in the number of incident severity classification
The Japan Council for Quality Health Care classifies level 0 and 1 incidents as minor incidents, regarding these incidents as “errors that can be avoided”. The Council regards level 2 and 3a incidents as “intermediate errors” and incidents above level 3b as “serious errors” 9). The number of incidents was highest in the fiscal years 2018 (27 cases) and 2017 (26 cases). Thereafter, 17, 10, nine, and six cases were observed in 2019, 2020, 2021, and 2022, respectively (Figure 1). Statistical analysis revealed that the decrease was significant after 2020 (2020: p < 0.01, 2021–2022: p < 0.001). Among the total 95 incident reports, 31 cases (33%) were level 0, 56 cases (59%) were level 1, two cases (2%) were level 2, six cases (6%) were level 3a, and no accidents above level 3b were observed. Level 1 incidents in particular decreased significantly after 2021 (2021: p < 0.05; 2022: p < 0.01; Figure 1); in addition, the chi-square test and residual analysis revealed no significant changes in the remaining levels.
The number of medical services in which incidents occurred before and after ISO 15189 implementation
Next, of the total 95 incidents, we analyzed the number of medical services in which incidents occurred. We compared the change before (2017 and 2018) and after (2019 to 2022) the implementation of ISO 15189 and observed that most of the incidents occurred during laboratory tests (i.e., hematological, microbiology, and clinical chemistry and immunology tests; transfusion tests; urinalysis, and body fluid tests) and not during physiological tests (Figure 2). Notably, the incidents related to night shift or day duty were highest in 2017–2018 (21 cases) but dramatically decreased in 2019–2022 (10 cases). In addition, physiological tests and clinical chemistry and immunology tests appeared to decline significantly (p < 0.05) between 2017–2018 and 2019–2022.
Incidents in each medical service by laboratory testing step
We further analyzed the number of incidents by laboratory testing step in each medical service (Figures 3 & 4). Of the total number of incidents, the number of incidents in pre-examination, examination, and post-examination processes was 46, 31, and 18 cases, respectively (Figure 3). The proportions of incidents in each process were relatively similar to those in a previous report 10). We observed that the incidents that occurred in blood collection and reception were mostly during pre-examination processes, whereas in clinical chemistry & immunology tests, incidents occurred mostly in post-examination processes. Despite the significant decrease in the total number of cases after 2020 (Figure 1), no significant change was observed in the trend in the proportions of incidents by laboratory testing step (Figure 4).
Analysis of recurrent incidents
Figure 5 shows the recurrent incidents among the total 95 incidents throughout the study period. We did not define “recurrence” as the same case of an incident but as the repetition of the same type of incident. The number of recurrent incidents was highest in 2018 (12 cases), and then gradually decreased (2019: 8 cases; 2020: 5 cases; and 2021: 1 case). Recurrences did not occur in fiscal year 2022. In summary, reducing recurrent incidents may take additional time, even with the application of ISO 15189 systems.
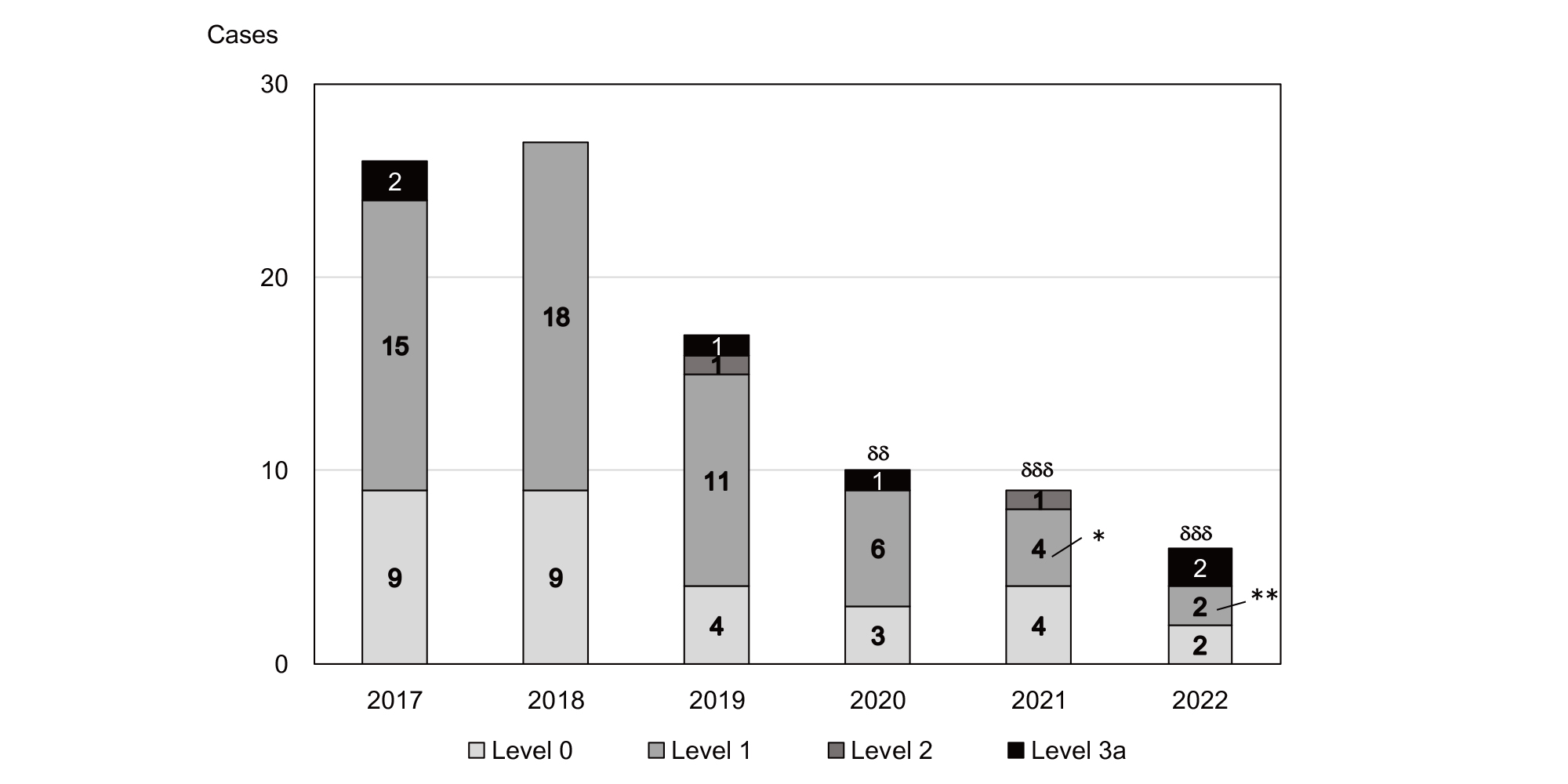
Figure 1 Number of incidents from 2017 to 2022 by incident severity.
The number of incidents in fiscal years 2017 or 2018 were compared with those in each year after 2019, using the chi-square test and residual analysis, and the statistical significance for the total number of incidents (δδ p < 0.01, δδδ p < 0.001) or each incident level (* p < 0.05, ** p < 0.01) was calculated. We used the Holm–Bonferroni method to calculate the revised p-value.
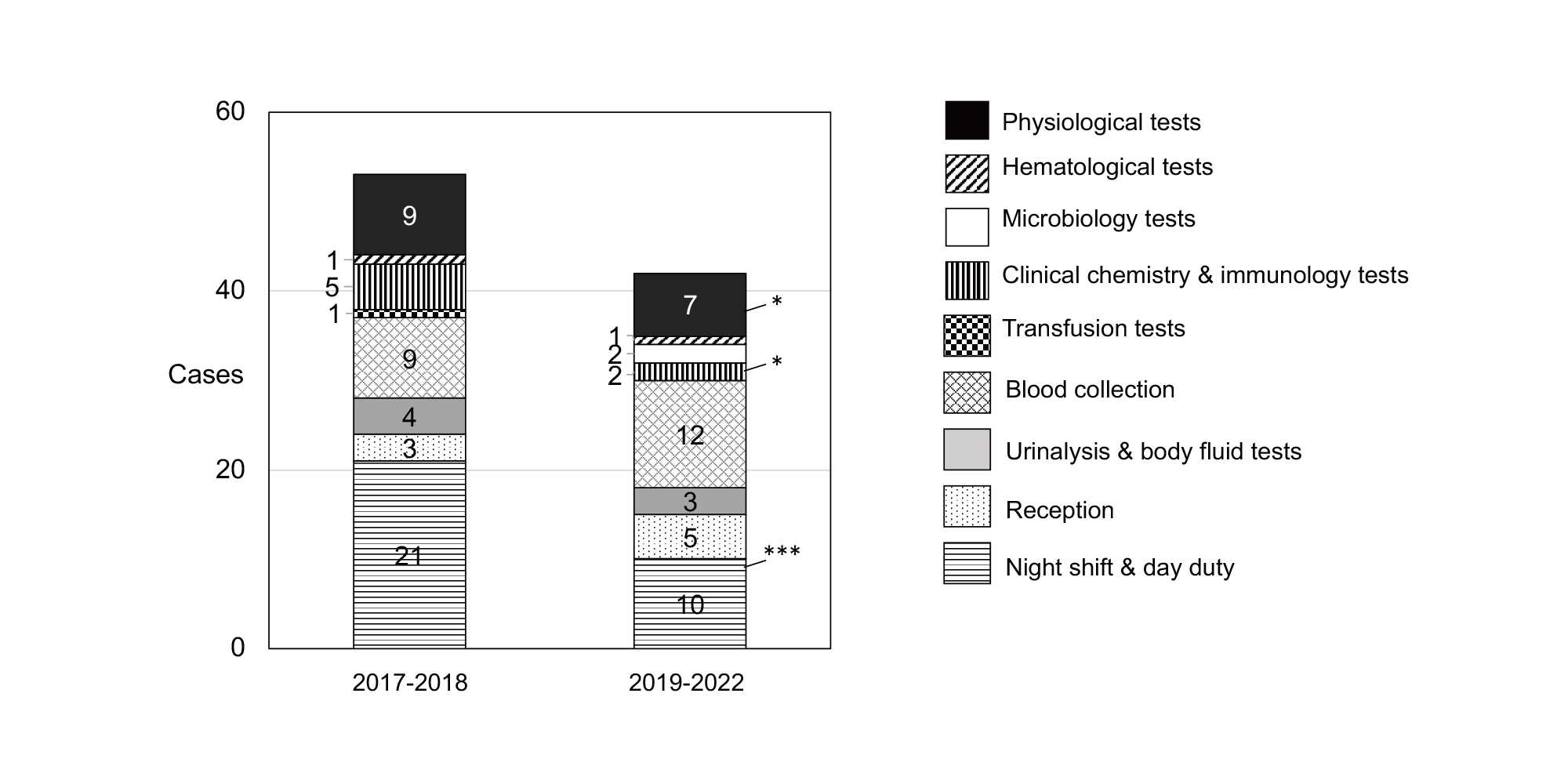
Figure 2 Number of incidents categorized by medical service in 2017–2018 and 2019–2022.
First, a cross-tabulation table that included incidents by medical service was prepared for the periods before 2017–2018 and after 2019–2022. Then the chi-square test and residual analysis were performed, and statistical significance was calculated. We noted the p-value, which was calculated from the adjusted residuals when significance was shown (* p < 0.05, *** p < 0.001).
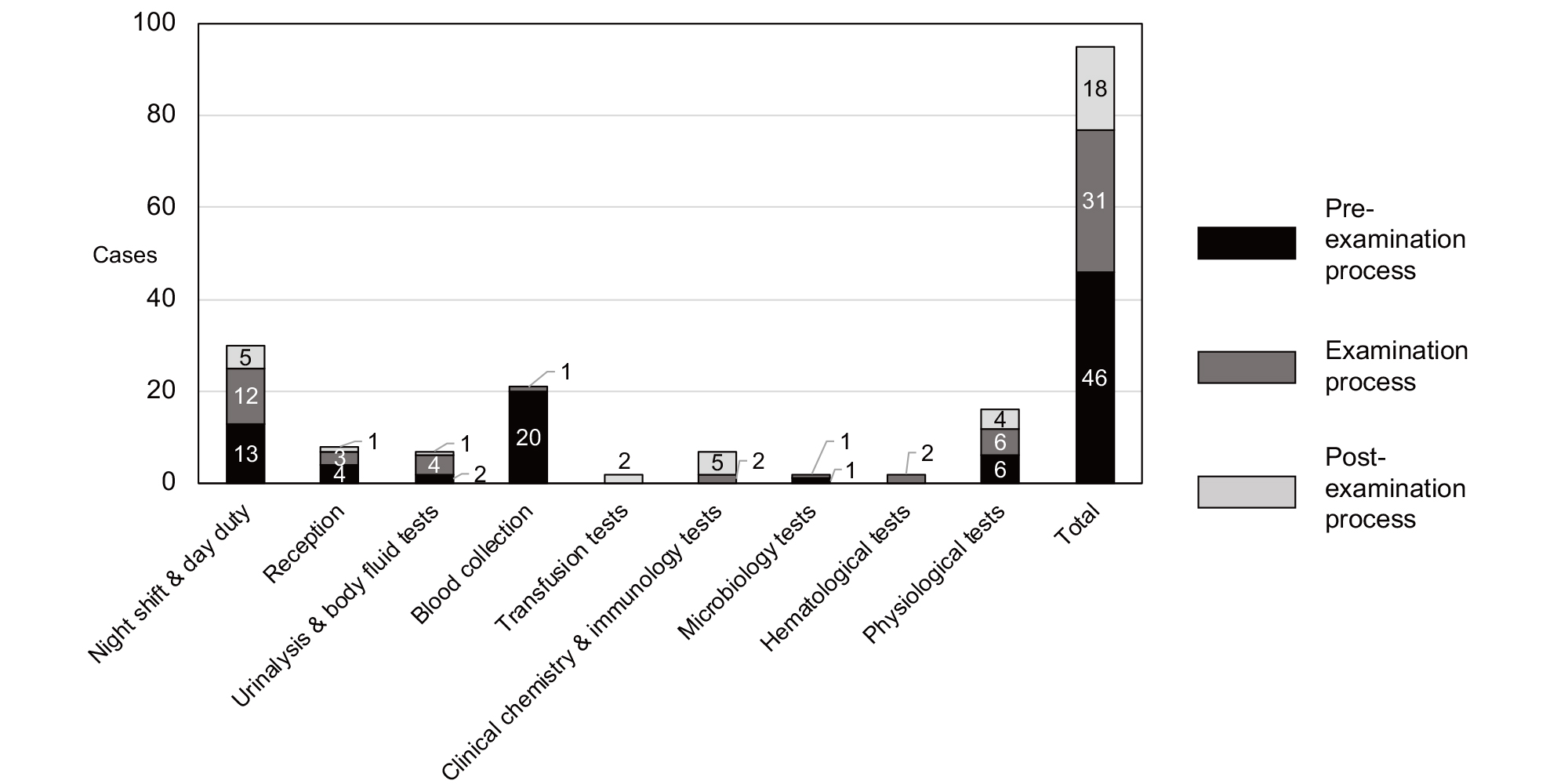
Figure 3 Total number of incidents categorized by examination process.
The total number of incidents that occurred in each medical service, categorized by examination process, is presented.
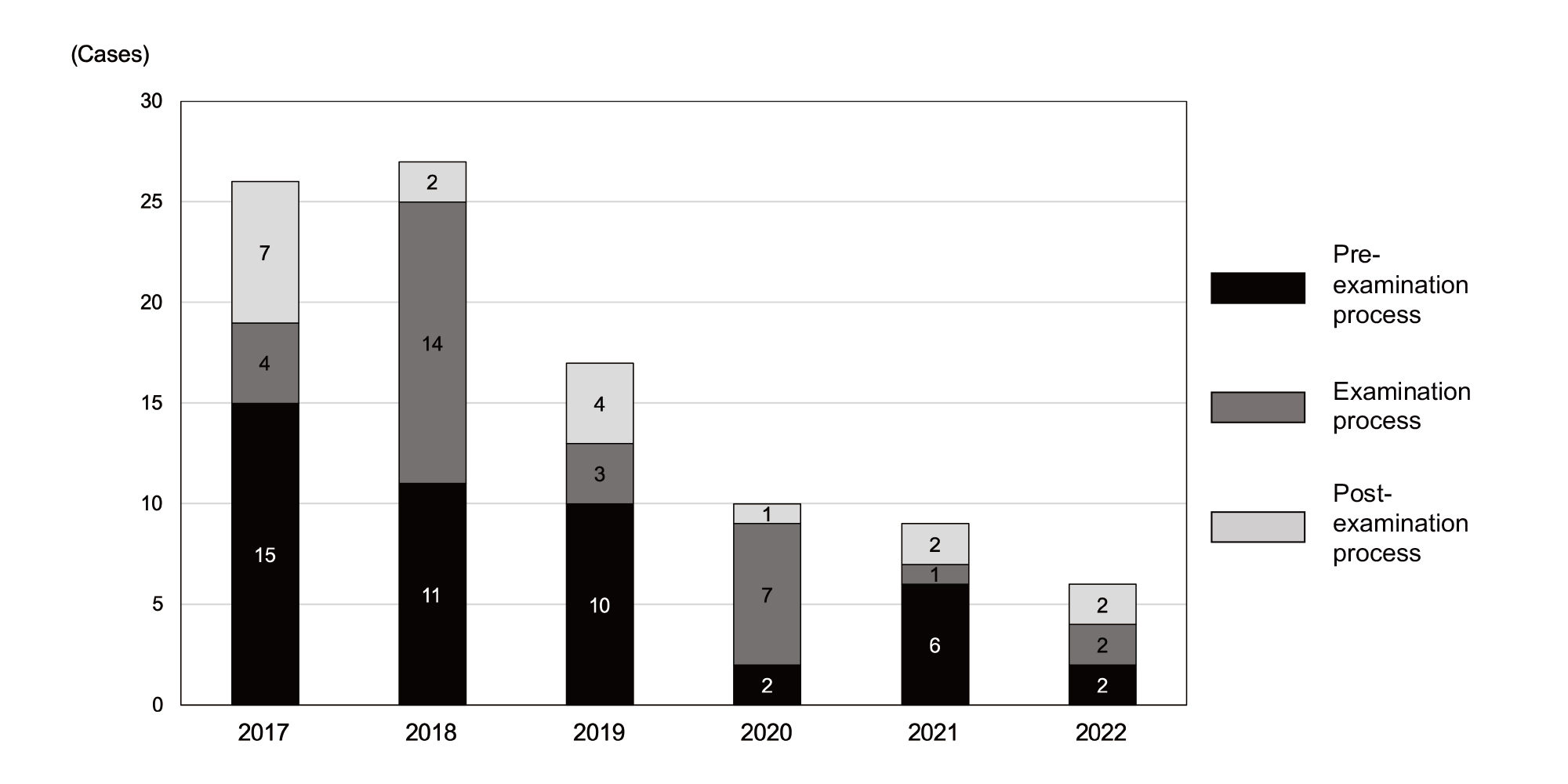
Figure 4 Number of incidents categorized by examination process from 2017 to 2022.
The number of incidents for fiscal years 2017 or 2018 was compared with that of each year after 2019, using the chi-square test and residual analysis. Statistical significance was calculated for examination processes, and no significance was found.
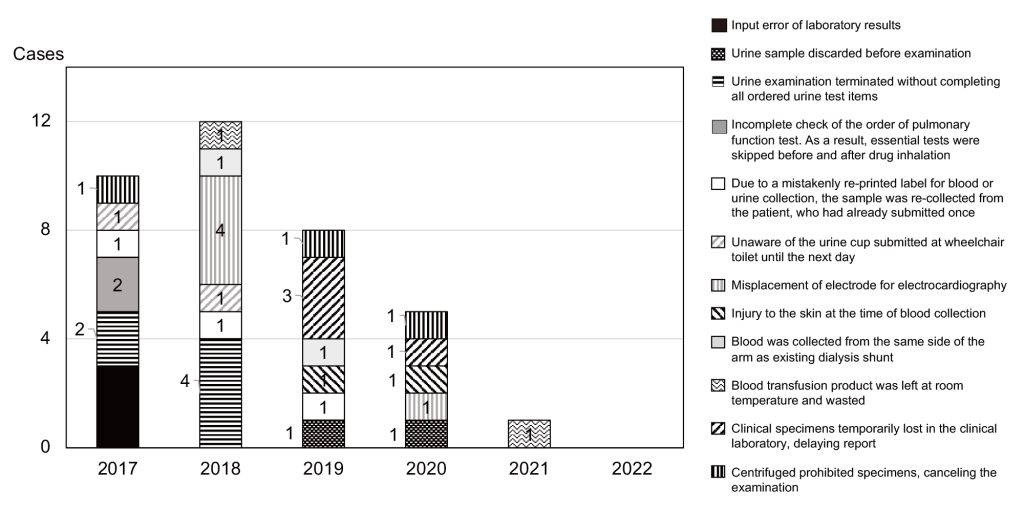
Figure 5 Number and type of recurrent incidents from 2017 to 2022.
The trends in the number and types of recurrent incidents are presented. No recurrent incidents were observed in 2022.
IV. Discussion
The ISO 31000 system is an international standard that corresponds to the JIS Q 31000 standard in Japan and is used as a risk management system. The ISO 31000 guidelines are centered on leadership and commitment. The effectiveness of risk management depends on the guideline’s integration into all aspects of an organization, including decision making. The remaining components of the framework are design, implementation, evaluation, and improvement. This approach is often represented in management literature as the plan-do-check-act cycle 11). In the ISO 15189 QMS management requirements, the following is listed as a general requirement: “The laboratory shall establish, document, implement, and maintain a quality management system and continually improve its effectiveness in accordance with the requirements of this international standard” 12). These concepts of design, implementation, evaluation, and improvement are consistent with those in the ISO 31000 risk management system. We observed an obvious decrease in the number of incidents after 2020, indicating that ISO 15189 was sufficiently effective as a risk management system. The relationships between ISO 15189 and 31000 are as follows. In 2019, ISO 15189 mainly consisted of “4. Management requirements” and “5. Technical requirements.” Risk management was only part of management requirement 4.14.6. In contrast, ISO 31000 provides a set of principles and guidelines for the design and implementation of a risk management framework and recommendations for the application of a risk management process 11).
ISO 31000 cannot be used for certification purposes, but guides internal or external audit programs. Organizations that use the standard can compare their risk management practices with an internationally recognized benchmark and have access to sound principles for effective management and corporate governance 13).
Recurrent incidents did not appear in 2022 (Figure 5). The number of new incidents significantly decreased after 2020, immediately after ISO 15189 implementation; however, the reduction of recurrent incidents may require additional time. Below, we discuss several possible causes of the decrease in recurrent incidents.
- The establishment of a process for informing everyone after incidents occurred: Before ISO 15189 implementation, an informing procedure was not available, and considerable time was required to notify the organization about incidents. However, after ISO 15189 implementation, an informing process was documented and disseminated. Furthermore, “incident sharing reports” allowed the staff to immediately share summaries of incidents, allowing a prompt analysis of causation and the identification of solutions. The establishment of this informing process improves risk management and may result in a reduction in the number of recurrent incidents.
- Establishment of an approach for root cause analysis: To allow root cause analysis and the development of incident prevention plans, we scheduled several corrective action workshops during the year.
- Development of complete prevention plans and corrective actions: We use an “improvement and prevention plan/report” when incidents occur. Written by a concerned and/or responsible person, this document describes the incident, its cause, and an improvement plan. Next, the document is approved and sometimes corrected by a technical manager who monitors technical aspects in the laboratory, a quality manager who monitors QMS, and a laboratory manager who develops and executes QMS operations. This series of detailed checks ensures the completion of corrective actions, contributing to the reduction of recurrent incidents.
Erroneous reports are known to occur frequently during day or night duty 14); our results are consistent with this finding (Figure 2). This is possible because, during day or night duty, the laboratory technologists who handle sample specimens usually perform physiological tests but not hematological or biochemical tests. Second, the laboratory technologists who usually handle sample specimens have insufficient skills to perform physiological tests such as electrocardiograms. In addition, during day or night duty, less-experienced laboratory technologists must promptly provide services without guidance. The implementation of ISO 15189 includes the preparation of standard operating procedures and day or night duty manuals, which may be especially useful for staff with day or night shift duty who are not familiar with procedures they do not regularly perform. In addition, we observed a significant reduction in incidents involving physiological and clinical chemistry and immunology tests (Figure 2). We cannot identify the reasons for the decline in immunology testing incidents. However, we estimate that the reason for the reduction in the number of incidences that involve physiological tests –– among which misplacement of electroencephalogram electrodes is frequent –– may be associated with our annual check of electrode placement, which may have negated the effect of personnel differences.
Heinrich’s law holds that for every workplace accident that causes a major injury, 29 accidents cause minor injuries, and 300 accidents cause no injuries 15). A similar analysis by Frank E. Bird in 1966 further supported the theory. Bird based his findings on 1,753,498 accident reports from 297 companies. His updated triangle showed the relationship between one serious injury accident and 10 minor-injury accidents, 30 damage-causing accidents, and 600 near-misses 16). Level 0 and 1 incidents can be regarded as “no injuries,” level 2 and 3 a incidents as “minor injuries,” and level 3b and higher incidents as “serious injuries.” Therefore, the 87:8:0 ratio obtained in our study roughly matched that in Heinrich’s law, suggesting that the CLIP system can efficiently detect near-miss incidents.
In conclusion, we analyzed incidents before and after the 2019 implementation of ISO 15189 and observed that the total number of incidents decreased significantly after 2020. In particular, level 1 incidents significantly decreased after 2021. We observed that incidents that occurred during the night shift and day duty declined dramatically after 2019. The proportions of incidents categorized by laboratory testing step remained unchanged. Overall, the implementation of a QMS that meets ISO 15189 standards is effective in reducing incidents.
Acknowledgments
We thank Anahid Pinchis from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This work was supported in part by the Shino-Test Corporation Research Fund.
Author contributions
R. Miura designed the study, collected and analyzed the data, and wrote the manuscript. R. Kozakai designed the study. S. Suzuki performed the statistical analyses. S. Takahashi wrote the manuscript. All authors have accepted responsibility for the entire content of this manuscript and have approved its submission.
Disclosure of Conflicts of Interest
None.
References
- Outline of revised health care low. Enforced on April, 2007. Downloaded from〈https://www.mhlw.go.jp/shingi/2007/11/dl/s1105-2b.pdf〉(accessed on May21, 2023)
- Kalra J. Medical errors: impact on clinical laboratories and other critical areas. Clin. Biochem 2004; 37(12): 1052-62.PubMed
- Tsunekawa K, Asai Y, Ikegami S, et al. lncident analysis and preventive measures taken in the general laboratory of hospital. Jap J Med Tech. 2019; 68(2): 333-8.J-STAGE
- Maeda F, Izumi S, Nakanishi H, et al. Efforts of inspection technology department and medical safety management committee: lncident accident report, positive report, fiscal year safety target. Jap J Med Tech 2017; 66(4): 404-10.J-STAGE
- Kayamori Y, Fujishima A, Noda(Inoue) N, et al. Approach for prevention medical test malpractice using ISO 15189. Rinsho Byori 2010; 58(8): 839-46.PubMed
- Shitara M, Umezu S, Katsuno H. Effects of the ISO 15189 accreditation on clinical laboratory. Rinsho Byouri 2009; 57(6): 521-6.PubMed
- Ohba Y, Kozakai R, Izumi Y et al. Efforts to gain accreditation for ISO 15189 in the department of clinical laboratory, Tohoku Medical and Pharmaceutical University Hospital. Rinsho Byori 2018; 66(12): 1341-7.
- Incident severity classification system recommended by the National University Hospital Council of Japan. Downloaded from〈http://nuhc.jp/wp-content/themes/NUHC/Portals/0/images/activity/report/sgst_category/safety/incidentcategory.pdf〉,(accessed on May 21, 2023)
- Itoh H, Usui R, Ikuno Y, et al. Disproportion of incident reports corresponding to each adverse effect on patients. J Shiga Univ Med Sci 2019; 32, 15-17.
- Astion ML, Shojania KG, Hamill TR, et al. Classifying laboratory incident reports to identify problems that jeopardize patient safety. Am J Clin Pathol, 2003; 120(1): 18-26.PubMed
- A Risk Practitioners Guide to ISO 31000: 2018. Downloaded from〈https://pdf4pro.com/view/a-risk-practitioners-guide-to-iso-31000-2018-60bdbe.html〉, (accessed on May26, 2023)
- ISO/TC212 National Committee. ISO 15189 Medical laboratories — Requirements for quality and competence, 3rd edition. Japanese Standards Association Group 2013; p.8-9.
- ISO 31000 risk management〈https://www.iso.org/iso-31000-risk-management.html〉(accessed on May26, 2023)
- Hashimoto T, Maki T, Futamura A, et al. Characteristics of 100 erroneous laboratory reports during a period of 8 years. Jap J Med Tech 2019; 68(3): 443-9.
- Heinrich HW. Relation of Accident Statistics To Industrial Accident Prevention. Proceedings of the Casualty Actuarial Society 1929; 16: 170-4.
- Bird FE Jr, Loftus RG. Loss control management. Institue Press; 1976. p19.